Varicocele repair
What is the varicocele?
Varicocele is found in approximately 35 % of infertile men who have never fathered a child and 81 % of men who were once fertile but are now infertile (secondary infertility).
Repair of varicocele will halt any further damage to testicular hormone function and in a large percentage of men, result in improved spermatogenesis, as well as enhanced Leydig cell function. The potentially important role of urologists in preventing future infertility underscores the importance of utilizing a varicocelectomy technique that minimizes the risk of complications and recurrence.
Diagnosis and treatment
Physical and ultrasound examinations for varicoceles are strongly recommended when an infertile male with abnormal semen characteristics visits an infertility clinic, as most evidence indicates that varicocele repair improves semen characteristics. Alternatively, early consultation with a urologist specializing in male infertility should be considered.
Operating method
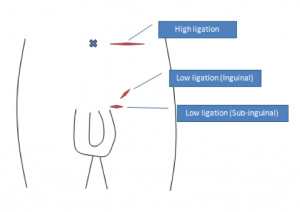
Among the several techniques available for varicocele repair, inguinal/ subinguinal microsurgical techniques are potentially the best in terms of effectiveness, complication rate, and recurrence rate. In our institution, we regularly perform microsurgical subinguinal varicocele repair.
First, about 3cm (1.5ich) skin incision will be made in the sub-inguinal area (see. Figure). Then, a spermatic cord will be exposed from incision and will be incised longitudinally to identify vessels and lymphatics.
Secondly, the artery will be dissected free of all surrounding tissue, tiny veins and lymphatics, using a microsurgical technique. The pulsation of suspected artery is evaluated by seeing a pulsating column of blood. Then, ligation of identified veins and lymphatics will be conducted with preservation of artery.
Potential complications
The most common complications from varicocelectomy are hydrocele, varicocele recurrence, and testicular artery injury (future atrophy of testis). Use of the operating microscope allows for reliable identification of spermatic cord lymphatics, internal spermatic veins and venous collaterals, and the testicular artery or arteries so that the incidence of these complications can be reduced significantly. Other complications can be an inflammation of wound, a hemorrhage around the incision, and an anastomotic leak.
Cost-effectiveness
With respect to cost-effectiveness, microsurgical varicocele repair under local anesthesia was the most costeffective treatment option; laparoscopic varicocele repair required expensive surgical materials and general anesthesia. In addition, varicocele repair for infertile men with abnormal semen characteristics allowed couples to reduce medical expenses related to childbirth by reducing the number of repeat IVF/ICSI cycles.
Summary
Despite the necessity for specific training in microsurgery, microsurgical varicocele repair, whether inguinal or subinguinal, is the most promising treatment option and is expected to become the gold standard for treating infertility in men with varicoceles.
Micro TESE
What is the non-obstructive azospermia?
Non-obstructive azoospermia (NOA) is a condition in which no sperm are present in the ejaculate because of severely abnormal sperm production. Most of these men have small-volume testes, elevated follicle-stimulating hormone (FSH), and empty epididymides. The general histologic patterns are found in men with non-obstructive azoospermia are Sertoli cell-only, maturation arrest and hypospermatogenesis.
Operating method
First, the scrotum skin will be cut to expose a testicle. After the testicular capsule has been opened, individual tubules are examined under approximately 20 to 25x magnification using microscope. The testicle will be inspected for the presence of a spermatogenically active region of normal seminiferous tubules, which containing many developing germ cells. Those tubules are usually larger and more opaque than tubules without sperm production, and therefore easily distinguishable from Sertoli cell-only, or sclerotic tubules that are much smaller in diameter.
Potential complications
Minor complications can be happen, such as an inflammation of wound and hemorrhage around the incision. In order to prevent hemorrhage, the wound will be pressured by tapes.
Summary
Sperm retrieval for use with the advanced form of assisted reproductive procedure of intracytoplasmic sperm injection (ICSI), is possible for many men with non-obstructive azoospermia. Men with NOA may have unique genetic defects that should be evaluated prior to an attempt at conception. At New York Hospital-Cornell, 58% of couples have sperm retrieved from the testis with TESE, and 55% of couples achieve a clinical pregnancy using sperm retrieved with TESE, using the advanced reproductive technique of ICSI.
Physician in charge
Masaki Kimura, M.D., Ph.D.
- Rank: Assistant Professor, Department of Urology, Teikyo University, Kaga, Itabashi-ku, Japan
- Training: Hirosaki University School of Medicine, Hirosaki, Aomori, Japan, 2002
- Residency: Kitasato University, School of Medicine, Sagamihara, Kanagawa, Japan, 2004-2008
- Fellowship: Duke University Medical Center, Durham, NC, USA, 2008-2011
- Clinical Interests:Male infertility, Sexual medicine, Prostate cancer